Medication Administration Record Sheet Form
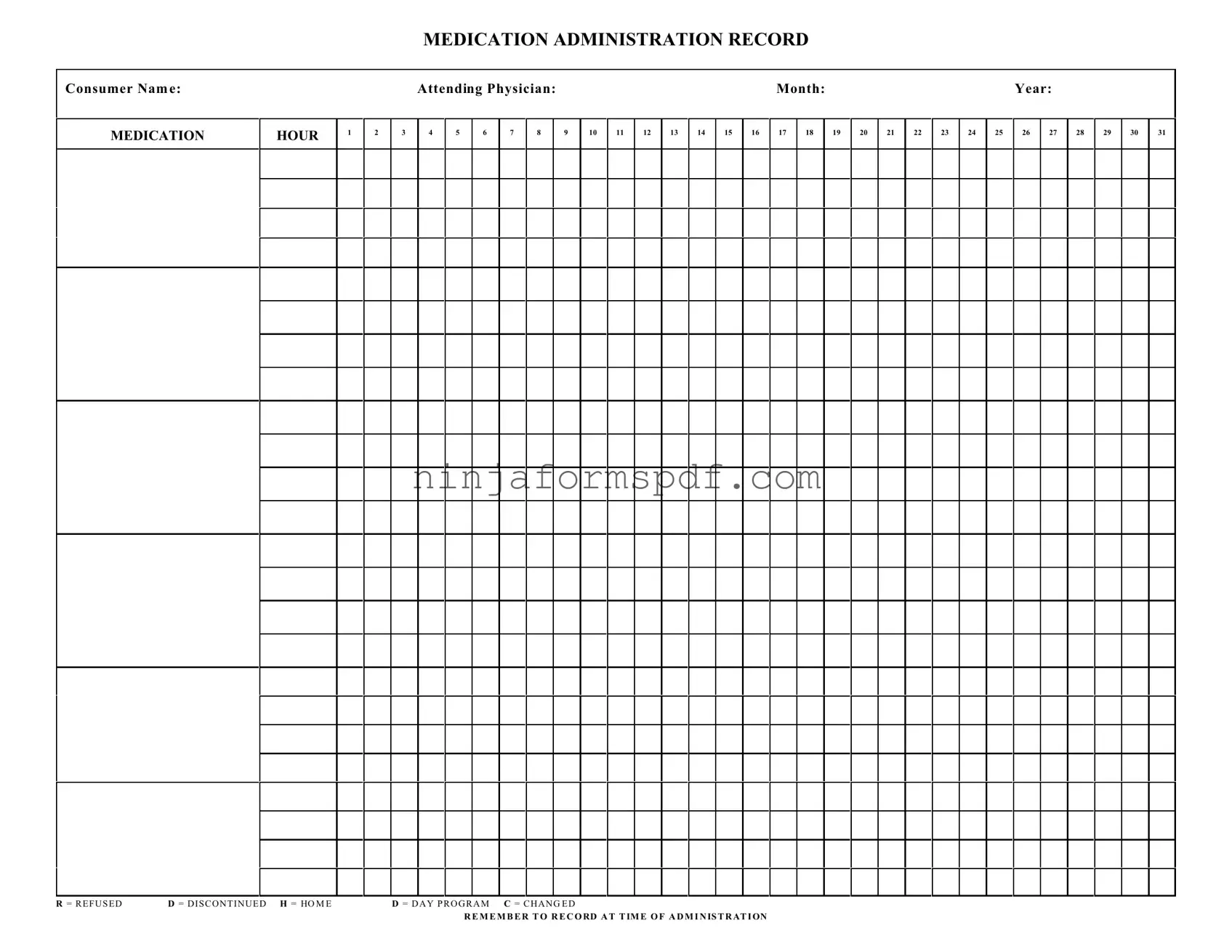
The Medication Administration Record Sheet is a crucial document meticulously designed to record and monitor the medication administered to a person over a given period. On this form, one can find various essential details, including the consumer's name, the attending physician, and spaces to mark medication administration across different hours of the day, meticulously listed from 1 through 31, reflecting the days of the month. It offers a comprehensive overview of medication schedules, dosage, and even provides options to denote when medication is refused (R), discontinued (D), if there has been a change (C), or if the medication was taken at home (H) or during a day program (D). This form is particularly invaluable in ensuring the health and safety of individuals by keeping a precise record of medication intake, allowing healthcare providers and caregivers to observe and adjust medication regimens as needed accurately. Additionally, it emphasizes the importance of recording medication administration at the time it is given, to maintain an unambiguous and real-time log of the individual's medication management.
Sample - Medication Administration Record Sheet Form
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
Form Information
| Fact Name | Description |
|---|---|
| Purpose of Form | Used to accurately record and track medication administered to an individual over a specified period. |
| Key Components | Includes sections for consumer name, medication hour, attending physician, and dates for administration tracking. |
| Recording Symbols | Utilizes symbols like R for refused, D for discontinued, H for home, and C for changed to note the medication status. |
| Importance of Timeliness | Emphasizes recording the administration at the time it occurs to ensure accuracy and reliability of the record. |
| Compliance and Legal Relevance | This form is essential for meeting healthcare regulations and standards, ensuring that medication administration is accurately documented. |
| Governing Laws | While this form is a standard tool in healthcare, specific governing laws may vary by state and setting, highlighting the importance of adherence to local regulations. |
Detailed Guide for Writing Medication Administration Record Sheet
Filling out the Medication Administration Record Sheet is an essential process to ensure that an individual receives the correct medications at the right times. It's crucial for tracking the administration of medications throughout the month. The form requires detailed information about the individual, the prescribing doctor, and a daily log of medication administration, including any changes in medication or if a dose was refused. Here’s a step-by-step guide to help you accurately complete this important document.
- Consumer Name: Start by entering the full name of the individual receiving the medication. Ensure spelling is correct to avoid any confusion.
- Attending Physician: Write the name of the physician who prescribed the medication. This is crucial for any follow-up or in case of an adverse reaction.
- Month: Indicate the month for which the medication is being recorded. Write the full name of the month to avoid any misunderstandings.
- Year: Enter the year to keep accurate records for future reference or audits.
- Under MEDICATION HOUR, you will see numbers 1 through 31, corresponding to the days of the month. Each day is divided into columns for recording medication administration at different hours.
- For each medication administration, record the time it was given next to the corresponding date. Make sure to do this at the time of administration to ensure accuracy.
- If a dose is refused by the consumer, mark an “R” in the appropriate column and day. It's important to communicate any refusals to the attending physician.
- If a medication is discontinued, use “D” on the days following its discontinuation. This helps in keeping track of medication changes and ensures that discontinued medications are not administered.
- For any medication taken while the consumer is at home (H), in a day program (D), or if there’s a change (C) in medication or dosage, document these details in the corresponding columns. This provides a comprehensive view of the medication routine.
- Remember to record at the time of administration, as mentioned at the bottom of the form. Timely documentation helps in maintaining an accurate and up-to-date medication record.
Completing the Medication Administration Record Sheet with attention to detail and accuracy is vital for the well-being and safety of the individual. This document also serves as an important tool for healthcare providers to monitor medication efficacy and adherence. Always double-check the information entered against the prescription details to ensure there are no discrepancies.
Important Points on Medication Administration Record Sheet
What is a Medication Administration Record Sheet?
A Medication Administration Record Sheet is a comprehensive document used to record all medications administered to an individual over a specific period, typically a month. It includes the consumer's name, medication details, dosage times, and attending physician's name. It provides a daily log for medication administration, tracking any changes, refusals, or discontinuations of medication.
How do I fill out the Medication Administration Record Sheet?
When filling out the sheet, record the medication name, dosage, and the specific time it was administered in the appropriate columns for each day of the month. If the individual refuses a medication, mark an "R" in the corresponding cell. For discontinued medications, use "D," and for changes in medication or dosage, mark "C." Always ensure to record the information at the time of administration to maintain accuracy.
What does "R," "D," and "C" stand for on the sheet?
On the Medication Administration Record Sheet, "R" stands for refused, indicating that the consumer declined to take the medication at the scheduled time. "D" signifies discontinued, meaning the medication was stopped, either temporarily or permanently. "C" represents a change in the medication regimen, whether a dosage adjustment or a switch to a different medication.
Who should complete the Medication Administration Record Sheet?
Healthcare professionals or authorized caregivers responsible for administering medication to the consumer should complete this sheet. This ensures that the individuals administering the medications are directly recording the administration details, maintaining an accurate and up-to-date record.
Why is accurate recording on this sheet important?
Accurate recording is crucial for maintaining the health and safety of the consumer. It helps in tracking the effectiveness of medications, identifying any adverse reactions, ensuring compliance with the prescribed medication regimen, and communicating important information among healthcare providers. Inaccuracies can lead to medication errors, which can have serious consequences.
What should I do if a medication is refused or discontinued?
If a medication is refused, mark an "R" for that day and time, and notify the attending physician as soon as possible to decide the next steps. For discontinued medications, mark a "D" and remove the medication from the administration schedule according to the physician's orders. Always follow up on any medication changes with the prescribing healthcare provider to ensure continuity of care.
Common mistakes
One of the common mistakes made when filling out the Medication Administration Record Sheet (MARS) involves the incorrect documentation of medication times. This form, crucial for tracking the administration of medications to individuals, requires precise recording of the time each medication is given. However, individuals sometimes mistakenly record the time they intend to give the medication rather than the actual time of administration. This error can lead to inconsistencies and inaccuracies in care records, potentially affecting the individual's health outcomes.
Another frequent error is the misinterpretation of the symbols used on the MARS. Symbols such as R for refused, D for discontinued, H for home, and C for changed are vital for indicating the status of each medication dose. However, individuals may not always be familiar with these abbreviations and, as a result, fail to use them correctly. This oversight can lead to a lack of clarity regarding the individual's medication regimen, causing confusion among care providers and ultimately compromising the individual's care.
Additionally, the failure to update the MARS in real-time is a common oversight. The instruction to "REMEMBER TO RECORD AT TIME OF ADMINISTRATION" is pivotal, ensuring that medication administration is tracked accurately. However, when care providers defer documentation until a later time, the risk of forgetting to record a medication dose increases. This gap in documentation can result in inaccurate medication tracking, potentially leading to medication errors or duplications.
Forgetting to include the attending physician's name and the relevant month and year at the top of the MARS can also lead to complications. These details are essential for ensuring the form is easily identifiable and appropriately filed, facilitating efficient communication between healthcare professionals and care continuity. Without this critical information, the risk of miscommunication about the individual's medication plan escalates, potentially impacting their treatment and care coordination.
Lastly, the omission of signatures or initials next to each recorded medication can compromise the integrity of the MARS. These signatures serve as a verification that the medication was indeed administered, providing an audit trail for accountability. When this step is overlooked, it raises questions about the authenticity of the medication records and can lead to doubts about the accuracy and reliability of the medication administration process.
Documents used along the form
The Medication Administration Record Sheet is a critical document in the management of patient care, particularly in settings where medications need to be tracked meticulously, such as hospitals, nursing homes, and by home health caregivers. To ensure comprehensive care and compliance with health regulations, several other forms and documents are often used alongside it. Each plays a vital role in maintaining patient safety and enhancing the quality of care.
- Physician's Medication Order Form: This document originates from a healthcare provider and authorizes the administration of certain medications to a patient, including dosages, frequency, and duration.
- Medication Reconciliation Form: Used to compare a patient's medication orders to all of the medications that the patient has been taking. This process is crucial to avoid medication errors, especially at transitions of care.
- Patient Consent Form for Medication: Records the patient's consent to receive the medications prescribed, acknowledging that they have been informed about the purposes, benefits, and potential side effects.
- Allergy Documentation Form: Lists any known drug allergies the patient has, which is paramount in preventing adverse drug reactions.
- Medication Incident Report Form: Completed when a medication error occurs, detailing the incident, the steps taken immediately after the discovery, and recommendations to prevent future occurrences.
- Controlled Substance Administration Log: Specifically used for tracking the administration of controlled substances, ensuring compliance with regulations related to narcotics and other controlled drugs.
- Pharmacy Communication Form: Facilitates communication between the healthcare team and the pharmacy, regarding medication orders, clarifications, and any adjustments needed.
- Medication Disposal Form: Documenting the disposal of medications ensures that drugs are disposed of properly and in a way that prevents misuse or harm to the environment.
Employing these documents in tandem with the Medication Administration Record Sheet provides a multi-layered approach to patient care. It ensures medications are administered safely, effectively, and in accordance with established healthcare policies. For healthcare providers, these tools are indispensable for delivering high-quality care and for maintaining thorough records that support both the well-being of patients and the operational integrity of the healthcare facility.
Similar forms
The Medication Administration Record Sheet is notably similar to the Patient Progress Notes used within various healthcare settings. Like the Medication Administration Record, Patient Progress Notes provide a chronological account, but focus on the patient's overall condition, including symptoms, medical interventions, and responses to treatment. Both documents serve as vital tools in monitoring a patient's care and ensuring consistency among healthcare providers, yet they differ slightly in focus—one on medication administration and the other on general health progress.
Another closely related document is the Nursing Shift Report. This report, handed over from one nurse to another at shift changes, summarizes patient care activities, including medications administered, which mirrors part of the Medication Administration Record Sheet's function. While the Nursing Shift Report encompasses a broader spectrum of patient care information, both documents are essential for providing continuous, informed care across different caregivers and time frames.
The Treatment Plan is also similar to the Medication Administration Record Sheet in its goal to outline a patient's healthcare strategy, yet it extends beyond just medication management. It covers diagnosis, goals, benchmarks, and interventions for a patient's healthcare journey. Both forms are pivotal in guiding and documenting the process and progress of care, offering a structured approach to achieving health objectives, with the Medication Administration Record focusing specifically on the medication aspect.
Lastly, the Patient Medication Profile bears resemblance to the Medication Administration Record Sheet by detailing the prescriptions a patient is taking. It typically includes medication names, dosages, and prescribing doctors, similar to sections of the Medication Administration Record. However, the Medication Profile serves more as a comprehensive list without the daily logging feature, highlighting the structured administration aspect of the latter. Both play crucial roles in preventing medication errors and ensuring the patient's safety.
Dos and Don'ts
When filling out the Medication Administration Record (MAR) Sheet, there are several important practices to follow to ensure the document is accurate and effective. Below are four recommendations on what you should and shouldn't do.
Do's:
- Ensure all entries are written in clear, legible handwriting to avoid any confusion or errors in medication administration.
- Record the administration of medication at the exact time it is given to accurately track and maintain the medication schedule.
- Include the full name of the medication, dosage, route of administration, and frequency as prescribed by the attending physician.
- Mark the appropriate box (e.g., R for Refused, D for Discontinued, H for Home, D for Day Program, C for Changed) accurately to reflect any changes or reactions regarding the medication administration.
Don'ts:
- Avoid making any alterations or erasures on the MAR Sheet without proper authorization and documentation explaining the reason for such changes.
- Do not use vague or unspecified terms for the medication or its administration details, as clarity is crucial for the safety and health of the consumer.
- Refrain from delaying the documentation of the medication administered. It should be recorded immediately to avoid any inaccuracies or oversight.
- Never guess or assume details about the medication or its administration. If unsure, consult with a healthcare professional or the attending physician before making an entry.
Misconceptions
Many individuals, including those in healthcare and those receiving care, have misconceptions about the Medication Administration Record (MAR) Sheet. Understanding these can help in ensuring the accurate administration and documentation of medication, which is crucial for patient safety.
- Misconception 1: The MAR Sheet is only for medical professionals.
This isn’t accurate. While the MAR Sheet is a tool primarily used by healthcare professionals to record administered medications, it also serves as a critical communication device for caregivers who may not have a medical background. Family members involved in the routine care of individuals, especially in a home setting, can and should understand how to read and record in the MAR Sheet under professional guidance.
- Misconception 2: All medication changes are immediately updated on the MAR Sheet by healthcare providers.
Although healthcare providers are responsible for updating the MAR Sheet, it's important to recognize that there may be delays. Communication lapses or changes in medication that occur during transitions in care (e.g., from hospital to home care) may not immediately be reflected. It requires diligent communication among all parties involved to keep the MAR Sheet current.
- Misconception 3: The MAR Sheet is just for tracking prescription medications.
Many assume the MAR Sheet is exclusively for prescription medications, but it also documents the administration of over-the-counter (OTC) medications, dietary supplements, and as needed (PRN) medications. This comprehensive approach ensures a full view of an individual’s medication regimen, helping to prevent interactions and side effects.
- Misconception 4: If a dose is missed, it should not be recorded on the MAR Sheet to avoid errors.
Contrary to this belief, it is crucial to document any deviations from the medication regimen, including missed doses, on the MAR Sheet. Noting these instances provides healthcare professionals with a complete history of medication administration, allowing for informed decisions concerning an individual’s care and necessary adjustments.
Key takeaways
Filling out and using the Medication Administration Record (MAR) Sheet form correctly is essential for ensuring the safe and effective administration of medications. The following key takeaways provide guidance on how to accurately complete and utilize this form.
- Consumer Identification: Always start by verifying the consumer's name on the MAR to ensure that the medication is administered to the correct individual. This is crucial for preventing medication errors.
- Medication Hour Tracking: The MAR includes columns for each hour of the day. It is important to record the administration of medication at the exact time it is given to accurately track adherence and timing.
- Attending Physician Information: Recording the name of the attending physician provides a reference for any questions or concerns regarding the medication orders.
- Month and Year: Clearly mark the month and year on the MAR Sheet. This helps in maintaining accurate medical records and facilitates easy retrieval of information when needed.
- Signatures for Administration: Each time medication is administered, the person administering the medication should sign or initial the MAR. This serves as proof of administration and helps in monitoring who administered the medication.
- Special Codes - R, D, H, C: Familiarize yourself with the special codes used in the MAR (R for Refused, D for Discontinued, H for Home, and C for Changed). Use these codes to accurately document any changes in medication administration or refusal by the consumer.
- Recording At Time of Administration: It is critical to record the administration of medication at the time it occurs rather than waiting until the end of the day. This practice reduces the risk of forgetting to document or making errors in recording.
- Documentation of Changes: If there are any changes in the medication orders, such as dosage adjustments or discontinuation, these changes should be documented promptly on the MAR Sheet.
- Review and Audit: Regular review and audit of the MAR Sheets are necessary to ensure compliance with medication orders and to identify any patterns of missed doses or refusals. This can help in addressing any underlying issues promptly.
Accurate and diligent use of the Medication Administration Record Sheet form is a vital part of medication management. It ensures that individuals receive their medications as prescribed and provides a clear record for healthcare providers, caregivers, and auditors. By following these key takeaways, users of the MAR Sheet can contribute to the safety and well-being of the consumers under their care.
Discover Other PDFs
CBP Declaration Form 6059B - It is available in multiple languages to accommodate international travelers and ensure clear understanding.
Fedex National - Space for shipper and consignee phone numbers, enhancing communication for delivery coordination.