DD 2870 Form
In the realm of military healthcare, the practical aspects of managing and sharing personal health information between providers, beneficiaries, and authorized parties are streamlined through specific forms and protocols. Among these, the DD 2870 form emerges as a crucial document designed to authorize the disclosure of personal health information. This form encapsulates a bridge between privacy and necessity, allowing military service members, their families, and other entitled individuals to facilitate the sharing of their medical records for varied reasons, including continued healthcare, insurance processing, or personal recordkeeping. The significance of the DD 2870 form is underscored by its stringent compliance with privacy laws and regulations, ensuring that sensitive health information is shared securely and only with explicitly authorized entities. As such, navigating the specifics of when and how to use this form, understanding the permitted scope of information disclosure, and complying with its procedural requirements are essential steps for those seeking to manage their healthcare within the military's extensive and complex healthcare system.
Sample - DD 2870 Form

Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
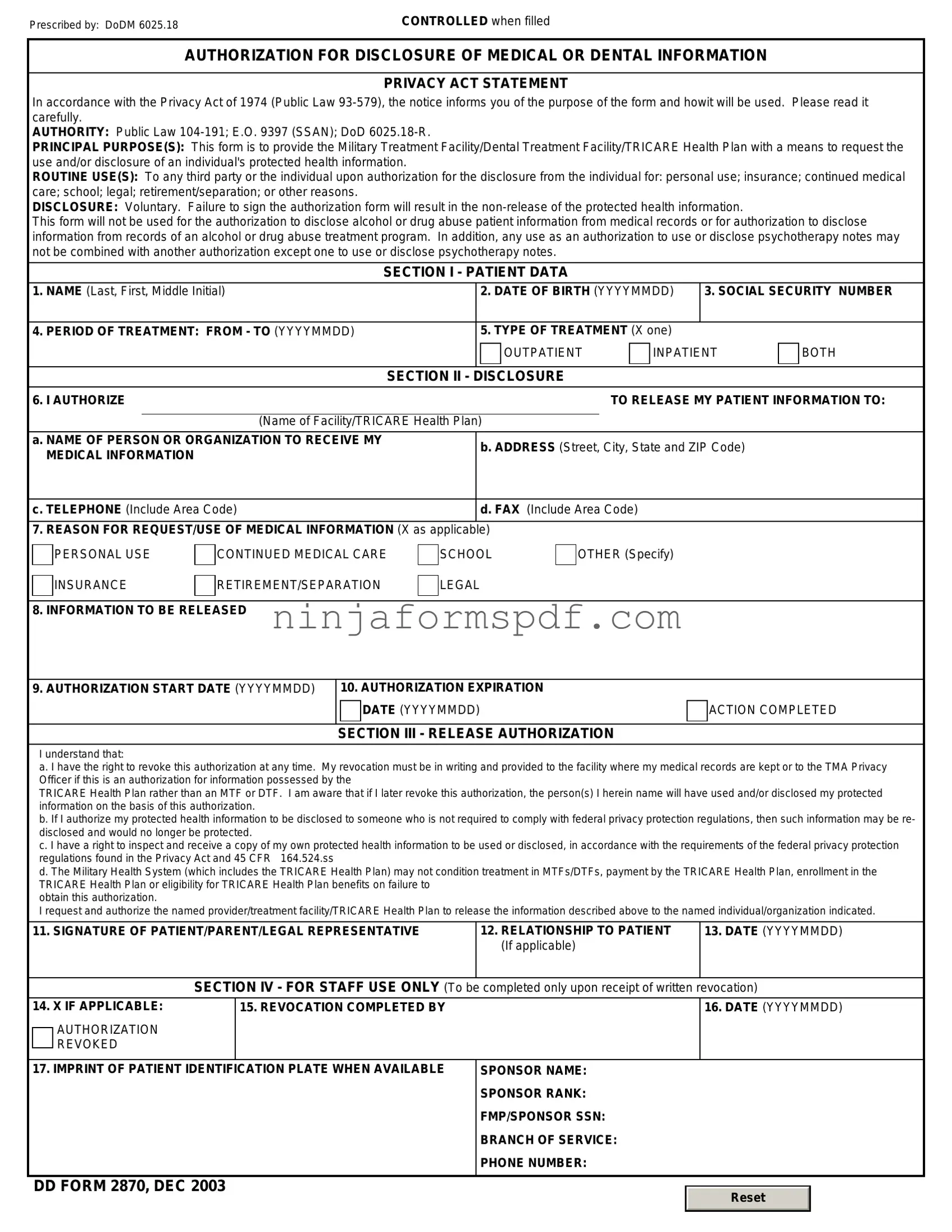
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Form Information
| Fact Name | Description |
|---|---|
| Purpose of DD 2870 | Authorization for Disclosure of Medical or Dental Information. This form allows the release of medical or dental records to authorized individuals, entities, or organizations. |
| Primary Users | Members of the military, veterans, and their families use this form to grant permission for the disclosure of their health information. |
| Requirement for Use | Completion and signature of the individual whose records are to be released or their legal representative are necessary for the form to be valid. |
| Governing Law | Federal privacy laws, notably the Health Insurance Portability and Accountability Act (HIPAA), dictate the terms under which medical information can be disclosed. State-specific laws may provide additional protections. |
Detailed Guide for Writing DD 2870
Completing the DD 2870 form is a critical step for individuals seeking to authorize the disclosure of their medical or dental records. This form serves as a formal request, ensuring that personal health information is shared in accordance with one's wishes, whether for ongoing medical care, insurance purposes, or personal use. Properly completing and submitting this form is not only about fulfilling a requirement; it's about taking an active role in managing one's healthcare journey, protecting privacy, and facilitating seamless communication between healthcare providers. The process involves a series of clear steps to ensure the form is filled out accurately and efficiently, allowing for a smooth transition of information as needed.
- Start by providing the name of the military medical or dental treatment facility (MTF/DTF) where the records are maintained. This should include the full address and contact details of the facility.
- Enter the patient's full name, including last, first, and middle initial, ensuring it matches the name under which the medical records are filed.
- Indicate the patient's Social Security Number (SSN) or Department of Defense (DoD) Identification Number to ensure proper identification and prevent any misplacement of records.
- For individuals filling out the form on behalf of the patient, state your relationship to the patient under "Authority for Release of Information." This helps clarify the legal right to access the patient's medical records.
- Specify the information to be disclosed. This section allows you to tailor the request to specific types of records or information, thereby protecting sensitive information that may not be relevant to the requestor.
- Clearly state the purpose of the disclosure, such as continuity of care, insurance claims, or personal use. Understanding the purpose helps the releasing facility adhere to privacy laws and regulations while providing the necessary information.
- Include any date restrictions, if applicable, to narrow down the search to records within a specific timeframe. This is particularly useful for historical information or when seeking records related to specific treatments or hospitalizations.
- Designate the name and address of the person or entity to whom the records should be sent. Ensuring this information is accurate prevents delays and ensures the records reach the correct destination.
- Review the section pertaining to patient rights, including the right to revoke the authorization. Understanding these rights is crucial for maintaining control over your personal health information.
- Date and sign the form, confirming the accuracy of the information provided and your authority to request the release of medical or dental records. If the patient is unable to sign, a legal representative may do so on their behalf.
After completing these steps, review the form carefully to ensure all information is correct and no sections have been overlooked. The completed DD 2870 form then should be submitted to the designated military medical or dental treatment facility. Submission can typically be done in person or mailed, depending on the facility's policies. Once received, the request will be processed, and the specified records will be prepared for release according to the details provided in the form. It's essential to follow up if confirmation of receipt or the status of the request is not received within a reasonable timeframe. Facilitating access to one's medical or dental records through the DD 2870 form is an important aspect of healthcare management, ensuring that individuals and their healthcare providers have the necessary information for optimal health outcomes.
Important Points on DD 2870
What is a DD 2870 form?
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, is used by military personnel, their families, and other authorized individuals to give permission for the release of their medical or dental records. This form is important for transferring records between facilities, allowing healthcare providers to share information, and for other purposes where medical or dental information needs to be disclosed.
Who needs to fill out the DD 2870 form?
Any individual who wishes to have their medical or dental records released to themselves, another healthcare provider, or an authorized person or organization will need to fill out the DD 2870 form. This may include members of the military, their dependents, or retired personnel seeking to share their records for ongoing medical care, insurance claims, or other personal or professional reasons.
How do I fill out the DD 2870 form?
Filling out the DD 2870 form involves providing your personal information, specifying which medical or dental records you want released, and identifying the person or organization to whom the records should be sent. You will also need to sign and date the form, indicating your consent for the disclosure. Make sure to read the instructions carefully to ensure all necessary fields are accurately completed.
Where can I submit the completed DD 2870 form?
The completed DD 2870 form should be submitted to the health information management department or the medical records office of the military facility where you received treatment. If you're unsure about where to send the form, contact the facility directly for further instructions.
Is there a fee to request medical or dental records with the DD 2870 form?
Typically, there is no fee for requesting your own medical or dental records for personal use or for them to be sent to another healthcare provider. However, fees may apply for extensive records requests or for copies intended for legal or insurance purposes. It's best to check with the facility handling your request for specific information regarding any potential costs.
How long does it take to process a DD 2870 form?
The processing time for a DD 2870 form can vary based on the facility's policies and the complexity of the record request. Generally, it can take from a few days to a few weeks. If your request is urgent, inform the facility, and they may be able to expedite the process.
Is my medical information safe when using the DD 2870 form?
Yes, your medical information is safe. The DD 2870 form ensures that your medical or dental records are only released with your consent and to authorized individuals or organizations. Military facilities take privacy and security seriously, following strict regulations to protect your health information during and after the transfer process.
Common mistakes
When individuals attempt to complete the DD 2870 form, a request for medical or dental records, errors can impede the process. One common mistake is not specifying the exact records needed. It's vital to detail the type of information required, such as medical histories, test results, or immunization records, to ensure the request can be processed efficiently and accurately. A lack of specificity may lead to unnecessary delays or the provision of incomplete information.
Another error frequently made involves incorrect or incomplete patient identification. The form requires precise information to accurately identify the individual whose records are being requested. This includes full name, date of birth, Social Security Number, and, if applicable, the military identification number. Failure to provide complete and accurate identification details can result in the rejection of the request, as the system relies on this information to locate the correct records.
The omission of an authorized signature often hinders the request process on the DD 2870 form. A signature from the individual making the request or their legal representative is crucial, as it signifies consent and authority to release the specified medical or dental records. Without this acknowledgment, healthcare entities are bound by privacy laws to withhold the information, protecting the individual’s confidentiality but potentially delaying necessary medical consultations or treatments.
Incorrectly identifying the recipient of the records is a further mistake that can lead to complications. The form requires clear details of where the records should be sent, whether it's to another healthcare provider, an insurance company, or the individual themselves. The address must be accurate and complete, including any specific department or individual's name if pertinent. Misdirection of records due to vague or incorrect recipient information can compromise privacy and lead to significant delays.
Last but not least, neglecting to specify the intended use of the requested information is a common oversight. Whether the records are needed for continuing care, insurance claims, or personal use, the purpose should be explicitly stated on the form. This not only helps in processing the request according to relevant privacy regulations but also in prioritizing the urgency and handling the records appropriately. Without this, the request may be processed in a standard, non-prioritized manner that does not align with the requester's needs.
Documents used along the form
When managing medical records or healthcare information within the military system, the DD 2870 form, Authorization for Disclosure of Medical or Dental Information, is a crucial tool. This form grants permission to release personal health information according to the guidelines set by the individual. However, this form does not stand alone. To ensure comprehensive management and accessibility of medical records, other forms and documents are often utilized alongside the DD 2870. Understanding these additional forms enhances the process of handling medical information efficiently and securely.
- DD Form 877: Request for Medical/Dental Records or Information. This form is used to request medical or dental records from military healthcare facilities. It's often required when service members need to transfer their medical records to civilian healthcare providers or when they need documentation for continuation of care.
- Standard Form 507 (SF-507): Clinical Record - Continuation Sheet. While not exclusively military, this form is used extensively within military healthcare facilities to document ongoing clinical information, follow-ups, and notes that exceed the initial documentation space. It complements the DD 2870 by providing detailed medical narratives and observations relevant to an individual's care.
- Privacy Act Release Form: Though not designated by a specific form number like the DD or SF forms, Privacy Act Release Forms are essential when handling personal health information. These forms are tailored to comply with the Privacy Act of 1974, allowing for a broader scope of information release under the appropriate circumstances.
- Health Insurance Portability and Accountability Act (HIPAA) Authorization Form: This authorization form is crucial for ensuring that the disclosure of health information complies with HIPAA regulations. Similar to the DD 2870, it grants permission to disclose health information, but it specifically addresses the privacy rules established under HIPAA, providing an added layer of legal protection and privacy.
Together, these documents form a suite of tools essential for the comprehensive handling of health information within the military system. Each plays a unique role in ensuring that service members' health information is managed respectfully, securely, and in line with all legal requirements. Whether transferring records, documenting care, or authorizing release of information, these forms and the DD 2870 are integral to the process.
Similar forms
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information form, serves a vital role in safeguarding patients' privacy while also allowing the necessary sharing of medical or dental records within specific, authorized circles. This form finds its counterparts in both the military and civilian realms, each designed with the privacy and consent of the individual at their core. Various documents across different sectors share key features with the DD 2870, illustrating the universal need for strict protocols in the handling of personal medical information.
The Health Insurance Portability and Accountability Act (HIPAA) Authorization Form is a civilian counterpart to the DD 2870. It allows patients to authorize the disclosure of their health information to designated individuals or entities. Like the DD 2870, the HIPAA form is heavily regulated to ensure the privacy and security of the patient's medical information, emphasizing the need for explicit consent before any sharing of personal health data.
The Release of Information (ROI) form used in civilian healthcare settings parallels the DD 2870. It permits healthcare providers to share a patient's medical records with other specified parties. The ROI form covers a broad range of information sharing, from medical history to treatment plans, similar to the DD 2870, which also facilitates a comprehensive exchange of medical data under authorized circumstances.
The Family Educational Rights and Privacy Act (FERPA) Release Form, while primarily focused on educational records, shares the consent-based release mechanism seen in the DD 2870 form. FERPA allows students or their guardians to authorize the disclosure of their educational records in a manner that mirrors the consent process for medical records, underscoring the importance of consent in information sharing across different types of personal data.
The Power of Attorney (POA) for Healthcare document, although broader in scope, relates closely to the consent aspect of the DD 2870. A POA for Healthcare grants a designated individual the authority to make healthcare decisions on behalf of someone else, potentially including the release of medical information, aligning with the DD 2870’s function of authorizing information sharing based on the patient's consent.
The General Consent for Medical Treatment form, required by many healthcare providers before delivering care, touches on the themes of the DD 2870 through its emphasis on informed consent. While it primarily focuses on treatment consent, it sometimes encompasses authorization for sharing medical information with other healthcare providers, paralleling the DD 2870's objective to facilitate the flow of necessary medical data under specific conditions.
The Social Security Administration's Authorization to Disclose Personal Information to a Third Party form resembles the DD 2870 in its purpose to share sensitive personal information with authorized entities. This document is essential for individuals who need to authorize the SSA to release personal information, echoing the DD 2870’s role in allowing the controlled dissemination of medical or dental records.
Finally, the Veterans Affairs (VA) Release of Information form is specifically tailored to veterans, authorizing the disclosure of medical records within the VA system or to external entities. This form mirrors the DD 2870 in its military context, providing a means for veterans to consent to the sharing of their medical information, similarly ensuring that such exchanges are conducted securely and responsibly.
In conclusion, the DD 2870 form shares fundamental characteristics with various authorization and consent forms across different sectors. Whether it's for medical, educational, or personal information, the underlying principle of these documents is the protection of individual privacy through consent. This commonality underscores the universal importance of respecting and securing personal data in all areas of administration.
Dos and Don'ts
When filling out the DD 2870 form, which is used to authorize disclosure of medical or dental information, there are several important dos and don’ts you should be aware of. This guidance helps ensure the process is completed correctly, safeguarding your privacy while allowing necessary information to be shared with designated individuals or organizations.
- Do read the instruction sheet carefully before filling out the form to ensure you understand each section and its requirements.
- Do print legibly in black or blue ink to ensure that all information is easily readable and to avoid processing delays.
- Do verify the recipient’s information, including their address and contact details, to ensure there are no delays in sending the information to the correct party.
- Do explicitly specify the types of medical or dental records you are authorizing for release, including dates of service, to prevent any unnecessary information from being shared.
- Don’t forget to sign and date the form; unsigned forms are invalid and will not be processed, leading to delays in the information release.
- Don’t leave any required fields blank. If a section does not apply, write “N/A” (for not applicable) to indicate that you have reviewed the section and determined it does not pertain to your request.
- Don’t ignore the expiration date of your authorization. Make sure the form will remain valid for the duration you need the information to be shared.
- Don’t provide incorrect information about yourself or the person you are authorizing to receive your information, as this can lead to violations of privacy or the release of information to the wrong individual or entity.
Correctly completing the DD 2870 form is crucial for ensuring that your medical or dental information is handled securely and shared appropriately. Following these dos and don'ts will help streamline the process and protect your personal information.
Misconceptions
The DD 2870 form, Authorization for Disclosure of Medical or Dental Information, is an important document but is often misunderstood. Let's address some common misconceptions.
It allows unlimited access to one's medical records: In reality, the DD 2870 form is designed to give specified individuals or organizations permission to access only the portions of your medical or dental records that you agree to release. The scope of access is controlled and does not equate to unlimited access.
It's only for military personnel: While it's commonly used within military circles, the DD 2870 form can also be relevant for civilians who are treated at military medical facilities. It's about the facility and the healthcare system, not just the patient's military status.
Signing it violates HIPAA protections: The Health Insurance Portability and Accountability Act (HIPAA) has comprehensive rules to protect patient privacy. The DD 2870 form is in compliance with HIPAA, as it requires explicit consent from the patient before any information is released, ensuring that the disclosure of medical or dental information is legally permissible.
The form is permanent: Consent given via the DD 2870 form is not indefinite. The form allows for the specification of an expiration date, until which the authorization is valid. After this period, a new form must be completed for continued authorization.
It's only for sharing information with external entities: While the form can be used to authorize disclosure to individuals and organizations outside of the Department of Defense, it's also used for sharing information between entities within the military health system. The purpose is to facilitate continuity of care within and outside the military network.
Completing the form is complicated: Although dealing with official forms can sometimes be daunting, the DD 2870 form is designed to be straightforward. Clear instructions are provided to guide the individual through the process of specifying what information can be shared, with whom, and for how long.
Electronic signatures are not allowed: Given the advancements in digital technology and to facilitate easier submission, electronic signatures are accepted on the DD 2870 form, provided they meet the specific requirements set by the relevant authorities.
Understanding the DD 2870 form correctly ensures that individuals can make informed decisions about disclosing their medical or dental information, maintaining their privacy while receiving the care and support they need.
Key takeaways
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, plays a vital role in managing the sharing of health records within military communities. Understanding how to correctly fill out and use this form ensures that individuals can efficiently share their health information with authorized parties, whether for medical care, billing, or administrative purposes. Here are four key takeaways to consider:
- Ensure Accuracy in Completing the Form: Accuracy is paramount when filling out the DD 2870 form. Individuals must provide precise and current information regarding their identification, including full name, date of birth, and social security number. This ensures that the correct medical or dental records are identified and shared according to the authorization.
- Specify the Purpose of the Request: Clearly outlining the purpose for disclosing medical or dental information is crucial. The form allows individuals to specify the reason for the request, which could range from personal use, continued medical care, to insurance claims. An explicit description prevents unauthorized access and ensures that the information is used appropriately.
- Define the Scope of Information to be Released: It’s essential to delineate the scope of information that is authorized for release. This might include specifying certain types of records (e.g., medical diagnostics, treatment history) or setting a time frame for the records in question. Limiting the scope helps protect privacy and ensures that only the necessary information is disclosed.
- Be Aware of the Expiration of Authorization: The authorization to disclose medical or dental records is not indefinite. The form requires a stated expiration date or event, after which the consent to share health information is no longer valid. Individuals should carefully consider this timeline to make sure it aligns with their needs and provides adequate time for the authorized parties to access the information.
Properly completing and using the DD 2870 form is essential for the secure and efficient exchange of medical and dental information within the military community. It empowers individuals to take control of their personal health information, ensuring it's used in their best interest while upholding confidentiality statutes.
Discover Other PDFs
How to Make a Payroll Check - For HR departments, it's an operational document that supports payroll audits, compliance checks, and reporting obligations.
Funds Available for My Stay - Advises on the inclusion of necessary documents, such as photos and fees, critical for application processing.
Ms Word Chart - Ideal for budgeting, where you can categorize expenses, incomes, savings, and investments, monitoring your financial health at a glance.