Annual Physical Examination Form
An Annual Physical Examination form serves as a comprehensive tool designed to capture a wide array of health information crucial for maintaining or improving an individual's well-being. This detailed form ensures that healthcare providers have a complete snapshot of a patient's medical history, current health conditions, and medication regimen, thus facilitating tailored medical advice and interventions. It collects basic personal information, including the patient's name, date of birth, and Social Security Number, which is essential for identification and record-keeping purposes. It also delves into specific health areas by asking about diagnoses, significant health conditions, current medications, allergies, immunizations, and screening results such as for tuberculosis (TB) and various cancers. Furthermore, the form addresses hospitalizations and surgical procedures, providing a thorough medical history overview. Part two of the form focuses on the general physical examination, evaluating vital signs, and the condition of various bodily systems to ensure a holistic health assessment. Additionally, it prompts discussions on health maintenance recommendations, potential activity limitations, and the use of adaptive equipment if necessary, ensuring a proactive approach to healthcare. Ultimately, the form acts as a critical instrument in preventive healthcare, helping individuals and healthcare providers stay a step ahead in managing health effectively.
Sample - Annual Physical Examination Form
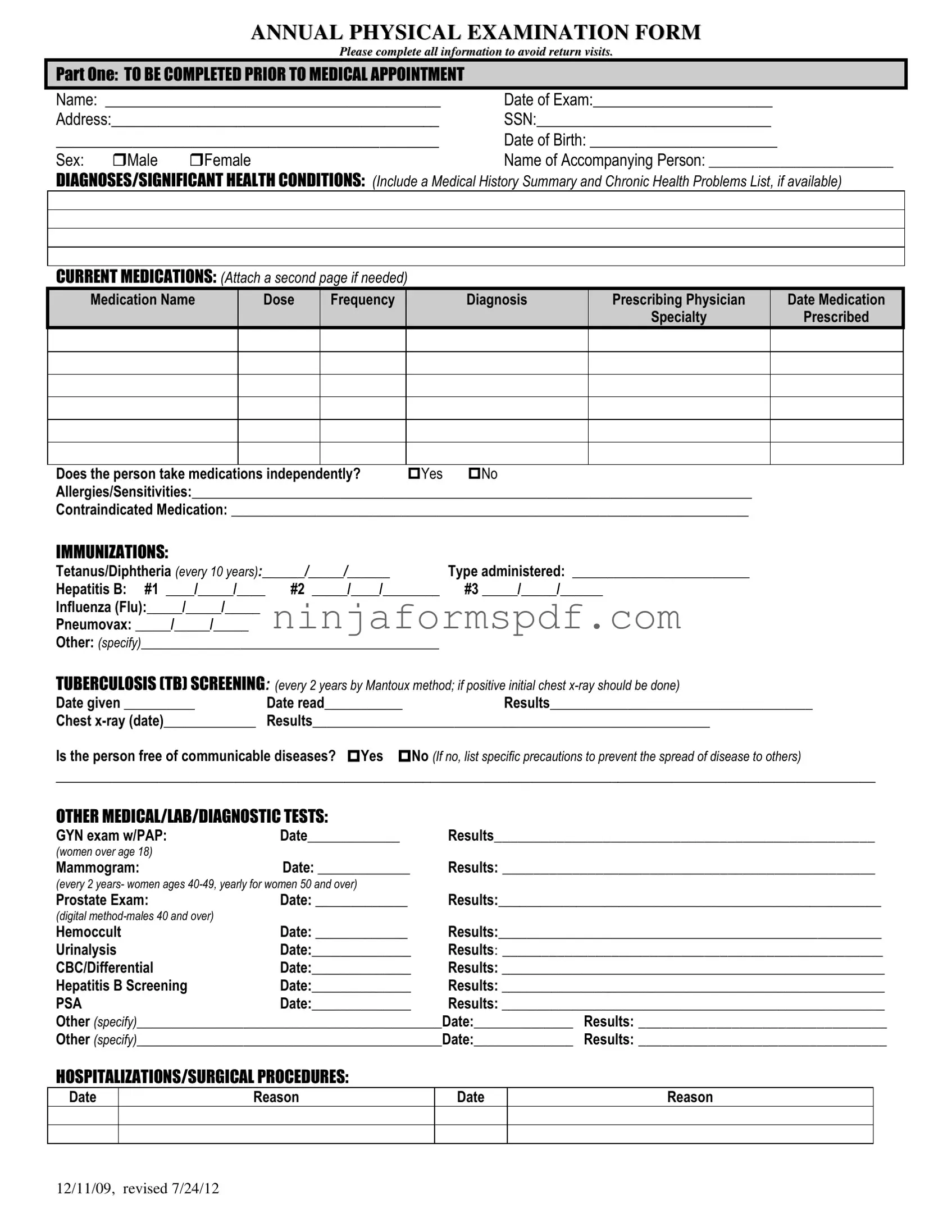
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12

PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
Form Information
| Fact Name | Detail |
|---|---|
| Completion Requirement | All sections of the form must be completed to prevent the need for return visits. |
| Medical History | Includes diagnoses/significant health conditions, current medications, allergies/sensitivities, and contraindicated medication. |
| Immunization and Screening | Records for Tetanus/Diphtheria, Hepatitis B, Influenza, Pneumovax, TB screening, and other specified immunizations are required. |
| Mandatory Testing | Includes tests like GYN exam with PAP (for women over 18), mammogram, prostate exam, Hemoccult, urinalysis, CBC/Differential, Hepatitis B Screening, and PSA among others. |
| General Physical Examination | Covers evaluation of systems including vision and hearing screening along with additional comments on medical history, medication changes, health maintenance recommendations, and needs for specialty consults. |
| Special Instructions and Considerations | Highlights recommendations for health maintenance, dietary needs, information for emergency situations, activity limitations or restrictions, use of adaptive equipment, and changes in health status from the previous year. |
Detailed Guide for Writing Annual Physical Examination
Filling out an Annual Physical Examination form is an essential step in managing your healthcare. It guides your healthcare provider in reviewing your health history, current condition, and determining any necessary follow-ups. This form, typically updated annually, plays a pivotal role in ensuring you receive comprehensive care tailored to your health needs. The process requires attention to detail and accurate information about your medical history, current medications, and any health concerns you might have. Below are the steps to fill out the form efficiently and accurately.
- Start by entering your Name, Date of the Exam, your Address, Social Security Number (SSN), Date of Birth, and Sex in the designated sections under Part One.
- If applicable, provide the Name of Accompanying Person.
- In the Diagnoses/Significant Health Conditions section, list any medical history summary, chronic health problems, and include a detailed list if you have it ready.
- Under Current Medications, accurately fill in the table with details about your medication, including the name, dose, frequency, and prescribing physician. Attach a second page if more space is needed.
- Specify if you take medications independently by checking Yes or No.
- List all known Allergies/Sensitivities and Contraindicated Medication.
- Update your Immunization records, providing dates and types for Tetanus/Diphtheria, Hepatitis B, Influenza, Pneumovax, and any other vaccinations received.
- Fill in the Tuberculosis (TB) Screening section with the date the test was given, read, the results, and any chest x-ray details if applicable.
- Answer whether the person is free of communicable diseases and list precautions if the answer is no.
- Under Other Medical/Lab/Diagnostic Tests, provide information on exams and screenings like GYN exams, mammograms, prostate exams, and others, including the dates and results.
- Record any Hospitalizations/Surgical Procedures with dates and reasons for each.
- In Part Two, for the General Physical Examination, register readings for blood pressure, pulse, respirations, temperature, height, and weight.
- Complete the Evaluation of Systems section by indicating whether normal findings were observed for each system listed and provide comments/descriptions where necessary.
- For Vision and Hearing Screenings, check whether the patient passed and if further evaluation by a specialist is recommended.
- Make additional comments regarding medical history, changes in medication, special medication considerations, recommendations for health maintenance, diet, emergency treatment information, limitations or restrictions for activities, and use of adaptive equipment.
- Indicate any change in health status from the previous year and specify if the individual is recommended for ICF/ID level of care, needs specialty consults, or has a seizure disorder, including the date of the last seizure.
- Ensure the physician’s name is printed, sign the form, and date it. Provide the physician’s address and phone number.
Completing the Annual Physical Examination form with diligence ensures that your healthcare provider has all the necessary information to assess your health comprehensively. This detailed approach contributes to a more personalized healthcare plan, aiding in the prevention, early detection, and management of potential health issues.
Important Points on Annual Physical Examination
What information should be completed before the medical appointment?
Before your medical appointment, you should complete parts concerning your personal information, which includes your name, the date of the examination, address, Social Security Number, date of birth, gender, and the name of any accompanying person. This section also asks for diagnoses or significant health conditions, a list of current medications (with an option to attach a second page if more space is needed), allergies/sensitivities, contraindicated medication, immunizations, tuberculosis screening, and any other medical, laboratory, or diagnostic test results. It's important to provide as complete a picture as possible to ensure accurate care and avoid the need for a return visit to complete missing information.
Which vaccinations and screenings are required?
The form requires updates on Tetanus/Diphtheria, Hepatitis B, Influenza, Pneumovax, and other vaccinations as specified by the individual or healthcare provider. Furthermore, a tuberculosis (TB) screening is requested every two years through the Mantoux method, with a chest x-ray required if the initial test is positive. This information helps in assessing your current immunization status and identifying any necessary updates to maintain health and prevent disease.
What information is asked about medications?
For medication, the form requires detailed information including the name of each medication, the dose, frequency of intake, the diagnosis for which it was prescribed, the prescribing physician's name, the medication's specialty, and the date it was prescribed. It also inquires whether the person takes medications independently. This comprehensive overview ensures that healthcare providers are fully informed about your medication regimen, which assists in preventing adverse drug interactions and ensuring the efficacy of treatment plans.
Are there specific tests and examinations for women and men?
Yes, the form specifies certain tests based on gender. Women over the age of 18 are asked to provide information on GYN exams with PAP smear results, and the guidelines for mammograms vary by age, recommending them every two years for women ages 40-49 and yearly for women 50 and over. For men, a prostate exam is advised for those 40 and over utilizing the digital method. These requirements help in early detection of potential health issues specific to each gender.
What should be listed under hospitalizations/surgical procedures?
Under hospitalizations and surgical procedures, the dates and reasons for any hospital stays or operations should be recorded. This history provides essential insights into past medical issues and interventions that might affect current health status or influence future medical decisions.
What is included in Part Two: General Physical Examination?
Part Two requires the completion of basic physical measurements like blood pressure, pulse, respirations, temperature, height, and weight. An evaluation of various systems such as eyes, ears, nose, mouth/throat, cardiovascular, musculoskeletal, and others is included, with an option to note the findings as normal or not, and space for additional comments. Information on vision and hearing screenings, with notes on whether further evaluation is recommended, is also requested. This comprehensive examination aims to give a holistic view of the individual's current health status.
How are changes in health status from the previous year documented?
Changes in health status from the previous year should be specified, including any new diagnoses, changes in medication, significant improvements or deteriorations in health conditions, or the development of new symptoms. This comparison to the previous year’s health status can provide valuable context for changes in health over time, indicating progress, recovery, or the emergence of new health concerns.
Common mistakes
Filling out the Annual Physical Examination form accurately is crucial for receiving appropriate health care, yet mistakes are common. One frequent error is not updating personal information, such as address or telephone number. This may seem minor, but up-to-date contact information is essential for any follow-up or in case of emergency.
Another common mistake is the omission of significant health conditions or medical history. Some might forget to list a past surgery or underestimate the relevance of a chronic illness. Providing a complete medical history is critical for a comprehensive medical evaluation.
When it comes to medication, many individuals fail to correctly detail their current prescriptions, dosages, and frequency. This oversight can lead to dangerous drug interactions or inadequate treatment plans. Similarly, not accurately reporting allergies or contraindicated medications can have severe consequences.
Immunization and screening test records are often neglected or inaccurately filled. These sections warrant special attention because they can prevent redundant testing and ensure that all preventive measures are up to date.
Some individuals mistakenly think that providing information about hospitalizations or surgical procedures is unnecessary if they occurred in the distant past. However, understanding a person's full medical history, including past hospital stays and surgeries, is vital for identifying patterns or potential complications.
Additionally, the part of the form that asks about family medical history often gets overlooked. Family health history can offer significant insights into potential health risks and genetic predispositions.
Forgetting to mention the use of any adaptive equipment or special aids is another error. This information is crucial for a complete view of the individual's daily functioning and any assistance they might require.
Lastly, many people neglect to indicate any changes in their health status since their last examination. Highlighting recent health developments, whether improvements or declines, enables healthcare providers to tailor care more precisely.
Documents used along the form
When it comes to staying ahead in health management, the Annual Physical Examination is a cornerstone document, ensuring that individuals receive a comprehensive assessment of their wellbeing. However, this form often works in conjunction with a series of other health-related documents to provide a full picture of an individual's health status. Below are several forms and documents that frequently accompany the Annual Physical Examination form, each playing a crucial role in maintaining and understanding one's health.
- Medical History Form: This document gathers comprehensive information about an individual's past health, including surgeries, illnesses, and family medical history. It's vital for detecting patterns that might be relevant to current health conditions.
- Immunization Record: Tracking vaccinations over a lifetime, this record ensures an individual is up-to-date with all necessary immunizations, helping to prevent the spread of infectious diseases.
- Medication List: A detailed account of all medications an individual is currently taking, including dosages and frequency. This is critical for monitoring potential drug interactions and understanding the overall treatment plan.
- Allergy Information Form: Identifies any known allergies to food, drugs, or environmental factors. It's essential for emergency situations and for planning appropriate medical treatment.
- Lab/Test Results: Documents such as blood work or imaging results provide objective data on an individual's health and are essential for diagnosing issues that might not yet present symptoms.
- Consent and Privacy Forms: Legal documents that protect privacy and denote an individual's consent to receive medical treatment. These are necessary for compliance with medical regulations and ensuring patient rights.
- Screening Questionnaires: Tailored to specific conditions or illnesses, these questionnaires can help identify risk factors or symptoms that warrant further investigation. They're an important tool in preventive health measures.
Together, these documents form a comprehensive toolkit that supports the Annual Physical Examination form. They ensure that healthcare providers have all the necessary information to offer personalized, effective care. Accurate and up-to-date documentation not only facilitates better communication between patients and healthcare professionals but also significantly enhances the quality of healthcare delivery.
Similar forms
The Pre-employment Health Questionnaire bears a resemblance to the Annual Physical Examination form by collecting health-related information that might affect an individual's ability to perform certain job duties safely. Like the Annual Physical Examination form, the questionnaire often requires information about past diagnoses, medication usage, and any ongoing health conditions. While the focus is on determining job fitness, both documents gather comprehensive health data to inform decision-making processes.
A Medical History Form found at a new patient's first visit to a healthcare provider is similar to the Annual Physical Examination form as it collects a wide range of health information. Both forms ask for a history of diagnoses, medications, allergies, and surgeries/procedures, facilitating a comprehensive review of the patient’s health status. The intention behind both documents is to ensure safe and personalized care by considering the individual's complete health background.
The School Physical Examination Form, required for students participating in sports or new enrollments, shares similarities with the Annual Physical Examination form. This form screens for any health issues that might impact a student's ability to safely participate in school activities. Both documents gather details on immunizations, past health conditions, and physical exam results, such as vision and hearing screening, to safeguard the well-being of the individual in an active environment.
The Travel Health Form required for international travelers by certain destinations or travel agencies is akin to the Annual Physical Examination form in its collection of health data to prevent the spread of diseases across borders. It typically inquires about vaccinations, recent illnesses, and the presence of chronic diseases similar to the comprehensive health overview provided by the Annual Physical Examination form. This ensures travelers are fit for travel and do not pose health risks to others.
The Disability Claim Form used when an individual files for disability benefits due to an inability to work because of health issues closely relates to the Annual Physical Examination form through its detailed collection of medical information. Both forms require data on diagnoses, treatments, medications, and the impact of health conditions on daily living. This thorough collection of health information aids in evaluating the claimant’s eligibility for disability benefits.
Dos and Don'ts
When preparing to fill out the Annual Physical Examination form, it is important to follow some basic guidelines to ensure accuracy and comprehensiveness. Here are eight dos and don'ts to consider:
- Do gather all necessary medical records before beginning. This makes it easier to provide accurate information about medical history, current medications, and past procedures.
- Do review the form thoroughly first to understand what information is required. This can help in collecting thoughts and ensuring that nothing is missed.
- Do use clear and legible handwriting if filling out the form by hand. This helps healthcare providers read the form without confusion.
- Do attach additional pages if needed, especially when listing current medications or detailing a complex medical history. Make sure these pages are securely attached and clearly labeled.
- Don't rush through the form. Take the time to fill out each section with care to prevent errors or omissions.
- Don't guess on dates or details. If unsure about specific dates (such as vaccinations or past procedures), it's better to verify this information with previous healthcare providers or records.
- Don't leave any sections blank unless they truly do not apply. If a section is not applicable, consider writing "N/A" to indicate that it was read but not skipped over.
- Don't forget to review and double-check the completed form before submitting it. This ensures that all information provided is accurate and complete.
Misconceptions
Several misconceptions surround the Annual Physical Examination form, which can lead to confusion and inefficiency in its utilization. Understanding these misconceptions is vital for patients and healthcare professionals alike, ensuring that the process is as effective and thorough as possible.
- Completing the Form Guarantees No Return Visits: A common misconception is that thoroughly completing the form will eliminate the need for any follow-up visits. While completing all sections can help streamline the appointment and reduce unnecessary follow-ups, it does not guarantee that further visits won't be necessary. The doctor might require additional information, tests, or consultations based on the initial findings during the physical examination.
- All Sections Are Equally Relevant for Every Individual: Another misconception is that every section of the form is directly relevant to every patient. The reality is that certain sections, such as specific screening tests or immunizations, may not apply to every individual. Recommendations for certain exams, like mammograms or prostate exams, are age and risk-factor dependent. Understanding the tailored nature of medical evaluations can help individuals better prepare for their examination.
- The Form Is Primarily for the Physician's Benefit: While it is true that the form provides vital information for the physician, thinking it serves only their benefit overlooks the patient empowerment aspect. By actively participating in filling out the form, patients can better understand their health, track significant changes, and prepare questions or concerns in advance. This active involvement can enhance communication and the overall effectiveness of the healthcare visit.
- Only Medical History and Current Medications Matter: While medical history and current medications are crucial components of the examination form, other sections are equally important. Elements such as allergies, immunization history, and information on any communicable diseases provide a comprehensive health overview, assisting in preventive measures and the management of existing conditions. Overlooking these sections can lead to incomplete care.
Clarifying these misconceptions ensures that individuals approach their Annual Physical Examination with realistic expectations and a clear understanding of the form’s scope and limitations. This clarity benefits both the patient and healthcare providers, fostering a more productive and informative examination process.
Key takeaways
Filling out an Annual Physical Examination Form correctly is crucial for ensuring comprehensive medical care. Here are key takeaways to keep in mind:
- Complete all sections before your medical appointment to prevent the need for a return visit. Double-check that you've filled out your personal information, including your name, date of birth, address, and Social Security Number.
- List all current medications, including dosage, frequency, diagnosis, and prescribing physician details. If more space is needed, attach a second page.
- Detail any diagnoses or significant health conditions, including medical history summaries and lists of chronic health problems, if available.
- Include information on allergies or sensitivities and any medications that are contraindicated for you.
- Update your immunization records. This includes vaccinations for Tetanus/Diphtheria, Hepatitis B, Influenza, and Pneumovax among others. Record the dates of each immunization.
- Report on Tuberculosis (TB) screening results and chest x-ray outcomes, especially if you have a history of positive TB screenings.
- Provide details of any recent hospitalizations or surgical procedures, including dates and reasons for each.
- During the General Physical Examination section, ensure accurate recording of blood pressure, pulse, respirations, temperature, height, and weight measurements, as well as evaluations of various body systems, vision, and hearing screenings.
- Pay attention to and accurately report on limitations or restrictions for activities, use of adaptive equipment, and any change in health status from the previous year.
- Clearly note if there's a need for further evaluation or specialist consultations, including any recommendations for health maintenance or changes in medication.
Properly completing the Annual Physical Examination Form can help your healthcare provider have a full picture of your health status, leading to better care and tailored healthcare recommendations.
Discover Other PDFs
What Is Immunization Records - Makes it easier to identify and address vaccine gaps, promoting higher immunization rates and healthier communities.
Odometer Disclosure Statement Indiana - Legal certification by a notary public of a vehicle's odometer reading, supporting transparent transactions.